
![]() [ main menu ]
[ previous page ]
[ main menu ]
[ previous page ]
Creutzfeldt-Jakob Disease: results of an inquiry in the fifteen Member States of the European Union
L Chambaud1, PWJ Peters 1, BC Merkel 2
1 Expert National Détaché, Commission Européenne;
Luxembourg
2 Agent temporaire, Commission Européenne; Luxembourg
Introduction
Creutzfeldt-Jakob Disease (CJD) was first described
in 1920-1921. CJD is a rare disease with a reported incidence
of 0.5 to 1 case per million people in Europe (1). This fatal
dementia belongs to the category of Transmissible Spongiform Encephalopathies
(TSE) whose human forms include Gerstmann-Sträussler-Scheinker
syndrome, kuru and fatal familial insomnia, all of which are very
rare. TSEs constitute “a group of subacute degenerative diseases
of the brain, caused by ëunconventionalí filterable
agents, with very long incubation periods and no demonstrable
inflammatory or immune response” (2). CJD occurs most often
in its sporadic form, although in about 10% of cases a genetic
origin can be found. CJD has also developed after organ transplants
or treatment with human growth hormone obtained from corpses infected
with the agent.
Some TSEs also affect animal species. The oldest
is Scrapie in sheep, which has been known in Europe since 1732.
This can also occur in other animals, such as minks, elks and
stags. Bovine spongiform encephalopathy (BSE) (3) was first described
in the United Kingdom in 1987. Since then BSE has spread among
British cattle, with the highest annual incidence reported being
36 681 confirmed cases in 1992. Concern has been growing about
the possibility of transmission between species, and particularly
of transmission of the agent from animals to humans (4).
A report in the Lancet of 6 April 1996
described 10 cases of new variant CJD (NV-CJD) discovered among
cases diagnosed in recent years in the UK. This led to a huge
crisis of confidence among the member states of the European Community
over the safety of beef. With regard to the aetiology of the cases,
the Lancet paper concluded, “That it is due to exposure
to the BSE agent is perhaps the most plausible interpretation
of our findings” (5).
The data available at European level have been
mainly collected by means of a collaborative surveillance project
established in 1993 which involves five member states: the UK,
France, Germany, Italy and the Netherlands. In order to obtain
information both on surveillance methods in Europe and on the
epidemiological data collected, the European Commission (Public
Health Unit) sent a questionnaire to the 15 member states. The
data presented here come from the responses to that questionnaire.
Methods
A questionnaire was sent to each member state
in April 1996. The recipients of the questionnaires were identified
by means of the member statesí official representations
to the European Community. All member states replied. To obtain
further detail, a second questionnaire was sent out in July 1996,
to which again all the states replied. This questionnaire sought
information on centres of expertise in the fields of epidemiology
and neuropathology, on the measures taken nationally to provide
information to consumers and to prevent the disease, and on data
on CJD since 1990. Only the replies on this last topic are presented
here.
Results
The data collected concern the surveillance
of CJD as a whole. The distribution of confirmed cases is set
out in table 1. The cases are presented by year of diagnosis.
When a case definition was detailed in the reply it was related
to the definitions developed by the five country collaborative
surveillance project mentioned above. This project drew a distinction
between possible cases (clinical indications), probable cases
(clinical indications and EEG evidence) and certain cases (cases
confirmed by standard neuropathological techniques and/or other
specific methods) (6).
| Pays/Country | 1990 | 1991 | 1992 | 1993 | 1994 | 1995 | 30 june 1996 | Case definitions |
| Allemagne/Germany | NA | NA | NA | 21(6m) | 39 | 48 | NA | Cas définis/Definite cases |
| Autriche/Austria | 5 | 6 | 4 | 8 | 9 | 10 | 6 | |
| Belgique/Belgium | 1.4 | NA | NA | 2.2 | 1.9 | 3 | NA | |
| Danemark/Denmark | Confirmation non disponible/No confirmation available | |||||||
| Espagne/Spain | NA | NA | NA | 14 | 13 | 7 | 1 | Cas définis/Definite cases |
| Finlande/Finland | 2 | 3 | 3 | 0 | 7 | NA | NA | |
| France/France | NA | NA | 50 | 45 | 60 | 62 | 24* | Cas définis et probables/Definite and probable cases |
| Grèce/Greece | Non disponible/Not available | |||||||
| Italie/Italy | NA | NA | NA | 37 | 33 | 41 | 21 | Cas définis et probables/Definite and probable cases |
| Irlande/Ireland | 0 | 2 | 0 | 0 | 0 | 1 | 1 | |
| Luxembourg/Luxembourg | NA | NA | NA | NA | 1 | 1 | NA | |
| Pays-Bas/Netherlands | NA | NA | NA | 9 | 8 | 5 | NA | Cas définis/Definite cases |
| Portugal/Portugal | 1 | 0 | 1 | 1 | 1 | 1 | 5 | |
| Royaume-Uni/United Kingdom | 31(6m) | 36 | 51 | 45 | 59 | 43 | 26 | Décès définis et probables/Definite and probable deaths |
| Suède/Sweden | Confirmation non disponible/No confirmation available |
NA: Non disponible / Non available * France: jusqu'au 30 mai 1996/ up to 30 May 1996
From table 1 it is clear that there was a lack
of consensus on the way to report confirmed cases in this survey
although a consensus definition is given in the collaborative
study; some countries included only certain cases, others both
certain and probable cases, and the UK reported deaths only, although
numbers of certain and probable cases have been published in that
country.
The diversity of definitions is reinforced
by table 2 on suspect cases. The questionnaire asked for data
on cases that were suspected but not confirmed. Some member states
provided all the cases referred to the surveillance unit, whether
or not they had been investigated; others took as the only criterion
the presence of clinical indications; still others included the
presence of a characteristic EEG; Austria did not report suspected
case; finally, some countries used the death certificate as a
criterion without providing any other details.
| Pays/Country | 1990 | 1991 | 1992 | 1993 | 1994 | 1995 | 30 june 1996 | Case definitions |
| Allemagne/Germany | NA | NA | NA | 13 | 37 | 40 | NA | Cas probables et possibles/Probable and possible cases |
| Autriche/Austria | Non enregistré / Not registered | |||||||
| Belgique/Belgium | 14* | NA | NA | 13** | 11** | NA | NA | Certificats de décès / Death certificates |
| Danemark/Denmark | 3 | 4 | 6 | 2 | 4 | 3 | NA | Certificats de décès / Death certificates |
| Espagne/Spain | NA | NA | NA | 10 | 10 | 9 | 8 | Cas probables et possibles / Probable and possible cases |
| Finlande/Finland | 1 | 2 | 0 | 2 | 0 | NA | NA | Critères cliniques / Clinical criteria |
| France/France | NA | NA | 8 | 11 | 11 | 15 | 11 | Cas possibles / Possible cases |
| Grèce/Greece | Non disponible/Not available | |||||||
| Italie/Italy | NA | NA | NA | 11 | 27 | 11 | 9 | Référés au registre national / Referrals to the national registry |
| Irlande/Ireland | 2 | 3 | 0 | 1 | 0 | 0 | 0 | Critères cliniques et EEG / Clinical criteria and EEG |
| Luxembourg/Luxembourg | NA | NA | NA | NA | 0 | 0 | 1 | Critères cliniques / Clinical criteria |
| Pays-Bas/Netherlands | NA | 2 | 1 | 4 | 10 | 3 | NA | Cas probables et possibles / Probable and possible cases |
| Portugal/Portugal | 6 | 3 | 2 | 5 | 4 | 3 | 1 | Cas cliniques en cours de révision / Clinical cases presently under revision |
| Royaume-Uni/United Kingdom | 52 | 75 | 96 | 78 | 115 | 85 | 56 | Référés à l’unité de surveillance CJD / Referrals to CJD surveillance unit |
| Suède/Sweden | 13 | 6 | 5 | 9 | 10 | NA | NA | Certificats de décès / Death certificates |
* Pays entier / The whole country ** Communauté flamande / The Flemmish community
Table 3 further strengthens the case for data
to be presented in a standard form. In effect some member states
calculate incidence on the basis of suspected cases, others on
the basis of confirmed cases. There is no clear trend in the incidence
of CJD in any of the countries able to supply data on incidence
rates since 1990.
| Pays/Country | 1990 | 1991 | 1992 | 1993 | 1994 | 1995 | Numérateur / Numerator |
| Allemagne/Germany | NA | NA | NA | 0.6 | 0.7 | 0.9 | Cas définis et probables / Definite and probable cases |
| Autriche/Austria | 0.7 | 0.8 | 0.5 | 1 | 1.1 | 1.25 | Cas confirmés / Confirmed cases |
| Belgique/Belgium | 1.4 | NA | NA | 2.2 | 1.9 | NA | Cas suspects / Suspected cases |
| Danemark/Denmark | 0.6 | 0.8 | 1.2 | 0.4 | 0.8 | 0.6 | Cas suspects / Suspected cases |
| Espagne/Spain | NA | NA | NA | 0.6 | 0.6 | NA | Cas suspects et confirmés / Suspected and confirmed cases |
| Finlande/Finland | A calculer / To be calculated | ||||||
| France/France | NA | NA | 0.85 | 0.8 | 1 | 1 | Cas définis et probables / Definite and probable cases |
| Grèce/Greece | Non disponible/Not available | ||||||
| Italie/Italy | NA | NA | NA | 0.7 | 0.6 | 0.7 | Cas confirmés / Confirmed cases |
| Irlande/Ireland | 0.6 | 0.9 | 0 | 0.3 | 0 | 0.3 | Cas suspects / Suspected cases |
| Luxembourg/Luxembourg | NA | NA | NA | NA | 2.5 | 2.5 | Cas confirmés / Confirmed cases |
| Pays-Bas/Netherlands | NA | NA | NA | 0.6 | 0.55 | 0.3 | Cas confirmés / Confirmed cases |
| Portugal/Portugal | 0.7 | 0.3 | 0.3 | 0.62 | 0.5 | 0.4 | Cas suspects / Suspected cases |
| Royaume-Uni/United Kingdom | 0.5 | 0.6 | 0.9 | 0.8 | 1 | 0.7 | Décès définis ou probables / Definite and probable deaths |
| Suède/Sweden | 1.5 | 0.7 | 0.6 | 1.1 | 1.2 | NA | Cas suspects / Suspected cases |
Only two member states (France and the UK)
have encountered NV-CJD and incorporated it in the data for confirmed
cases. Member states also differ in their policies on the inclusion
of other TSEs. Thus France, Germany and the UK include these familial
forms, but Austria and the Netherlands do not. France excludes
cases of iatrogenic CJD resulting from the use of human growth
hormone.
Discussion
Definitions used by the States vary, both for
confirmed and suspected cases and in how the incidence of CJD
is calculated. There are several reasons for the differences:
Several countries do not have yet a system
enabling suspected cases to be confirmed and rely entirely on
suspicions generated by death certificates.
Our questionnaire asked for suspected and confirmed
cases to be differentiated, whereas the definitions proposed in
the context of the five-state collaborative surveillance project
distinguished three different levels (possible, probable and
certain cases). Some of the disparities can therefore be explained
by different interpretations of the question. Different interpretations
of the term " suspected case " can partly
explain why some countries, such as France and Italy, have fewer
suspected than confirmed cases each year whereas with UK the reverse
is true (table 2). Moreover, the differences seen could be due
to different post mortem rates between countries leading to a
classification bias, affecting both confirmed and suspected cases
if other degenerative diseases (Alzheimerís, for example)
are wrongly diagnosed as CJD.
The annual incidences of CJD in member states
are generally between 0.5 and 1 case per million, the exceptions
being Luxembourg and Belgium and to a lesser extent Austria and
Sweden. However two points must be stressed:
The numerators used vary greatly depending
on the nature of the data available and how cases are understood
(suspected, confirmed or both).
Incidence is particularly inaccurate in countries
where very few cases arise each year. This is well illustrated
by the example of Luxembourg where one case each year produces
an incidence of 2.5 per million.
These partial explanations still leave real
doubts about the comparability of the data between member states.
Harmonisation of surveillance would be very valuable for a disease
whose reported incidence is very low and there would be clear
advantages in analysing the data at a supranational level.
It is difficult to see a clear trend in the
evolution of CJD since 1990 either in the total numbers or in
the incidence data. The fact that no increase is apparent must
be interpreted cautiously. Firstly it is difficult to verify that
the methods of data collection and of case confirmation in each
country have not changed since 1990. Secondly, in most countries
surveillance began only recently (only seven states can provide
data from 1992). Finally, a real increase could be disguised by
the lengthy periods between the appearance of the first signs
of the disease and its confirmation and between confirmation and
notification.
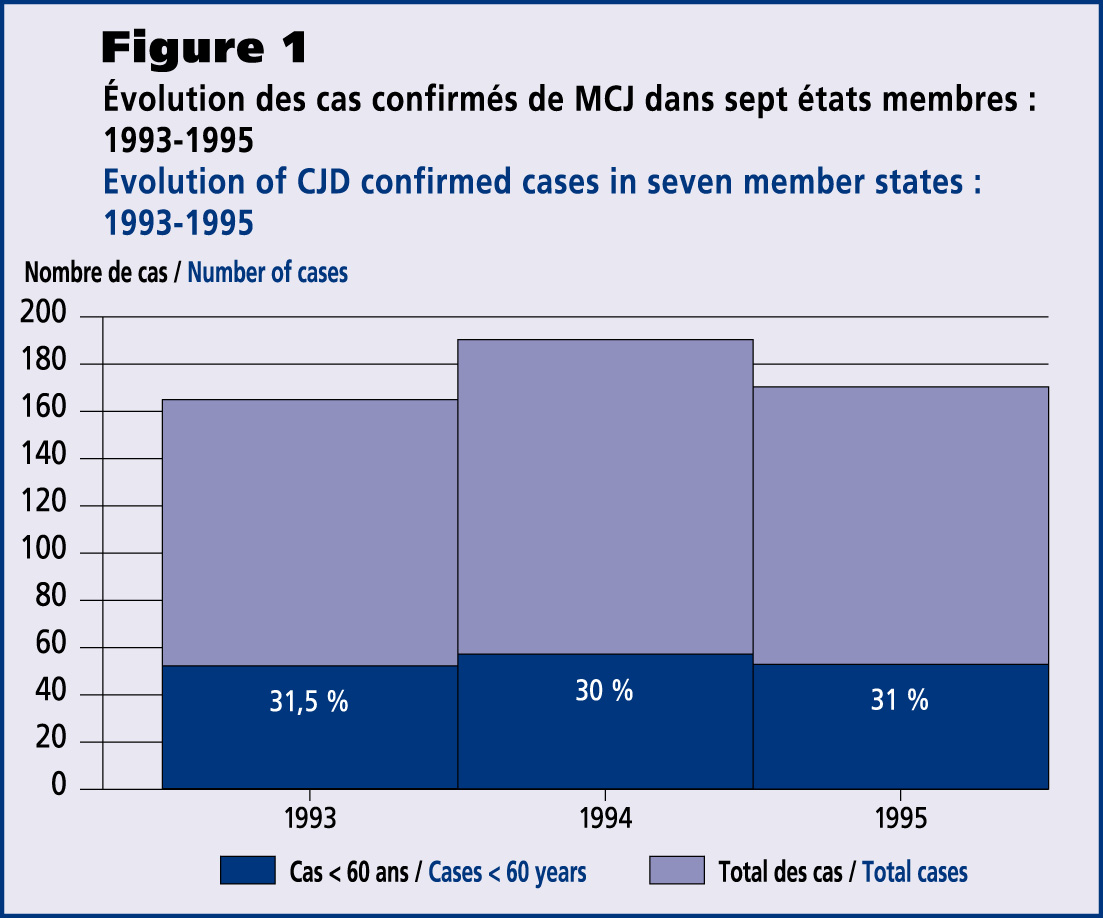
The data presented for 1993 to 1995 show no
change in the proportion of confirmed cases among people under
60 years of age. Cases of NV-CJD have been found among young people
(aged from 16 to 39 in the first published set). If the age criterion
remains, it will be important to be able to follow changes in
the number of cases in the youngest age groups throughout Europe.
In the light of this inquiry, it therefore seems indispensable:
to draw up common criteria for the fifteen member states both for the collection of information on CJD surveillance and for the analysis and diffusion of the results of this surveillance. Such coordination throughout Europe would enable the surveillance of the incidence of CJD and its different forms, including NV-CJD, and to detect any unusual trends in one or more countries. It could also help to calculate a baseline of expected cases both in Europe as a whole and in individual countries considering the very few cases diagnosed and notified each year. In addition, in the light of the work confirming the connections between BSE and NV-CJD (7), this surveillance should be closely linked to surveillance of animal TSEs.
to set up a study to examine in each member
state all the steps towards confirmation and notification of a
CJD case. This would clarify our understanding of the population
referred as suspected cases of CJD and enable the sensitivity
of the surveillance systems to be evaluated.
The questionnaire of this study is available
from the authors at the Commission of the European Communities,
DGV - F/21, Bât. J. Monnet, C4/107 Plateau du Kirchberg,
L 2920 Luxembourg.
References
1. Alperovitch A., Brown P., Weber T., Pocchiari M., Hofman A., Will R. Incidence of Creutzfeldt-Jakob disease in Europe in 1993. Lancet 1994; 343:918
2. Benenson A.S., Ed.: Control of Communicable Diseases Manual.. Washington: American Public Health Association, 1995
3. Patterson W.J.: Bovine spongiform encephalopathy and the public health. Journal of Public Health Medicine;17(3):261-268
4. Collee J.G.: BSE:stocktaking 1993. Lancet 1993; 342:790-3
5. Will R.G., Ironside J.W., Zeidler M., Cousens SN, Estibeiro A., Alperovitch A. et al. A new variant of Creutzfeldt-Jakob disease in the UK. Lancet 1996;347:921-25
6. World Health Organization. Division of Emerging and other communicable diseases surveillance and control: Report of a WHO consultation on clinical and neuropathological characteristics of the new variant of CJD and other human and animal transmissible spongiform encephalopathies. Geneva. WHO/EMC/ZOO/96.1
7. Collinge J., Sidle K.C.L., Meads J., Ironside
J., Hill AF. Molecular analysis of prion strain variation and
the aetiology of ënew variantí CJD. Nature
1996;383:685-90
![]()